Incorporating shared decision making in routine clinical practice: The missing link?
In 2017, Sarina Schrager and colleagues published a paper describing how shared decision making (SDM) for cancer screening decisions can be implemented in primary care settings. [1] It is freely available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5697707/ As of Sept 22, 2022 it has been cited 26 times according to Google Scholar .
Schrager and her colleagues explain that learning how to incorporate SDM into practice is important because it is a framework for providing the type of high quality care advocated in the Intitute of Medicine’s Crossing the Quality Chasm report that is “…respectful of and responsive to individual patient preferences, needs and values”. [2] They then describe three SDM models: the AHRQ SHARE method, the 5 A’s method described by the US Preventive Services Task Force, and the IAIS (Invite, Acknowlege, Instruct, Summarize) model.
They conclude that: “Practicing clinicians will need to choose a model that works well for their practice.”
Musings:
I thought this paper was notable for two reasons.
1: It clearly and simply explains why routine SDM for screening decisions is an important goal to pursue.
2: The conclusion highlights the importance of adopting a SDM practice that fits in the local practice context.
The latter point is consistent with the Canadian Institute for Health Research (CIHR) Knowledge to Action (KTA) Framework, originally described by Graham and colleagues in 2006. [3] The original paper has been cited 4,821 times according to Google Scholar on September 22, 2022, so clearly, there is a lot to learn about this idea.
For now, however, I’d like to focus on the basic structure the KTA framework provides for thinking about how research findings can be effectively used to improve clinical patient care.
The figure below shows the original framework [3] :
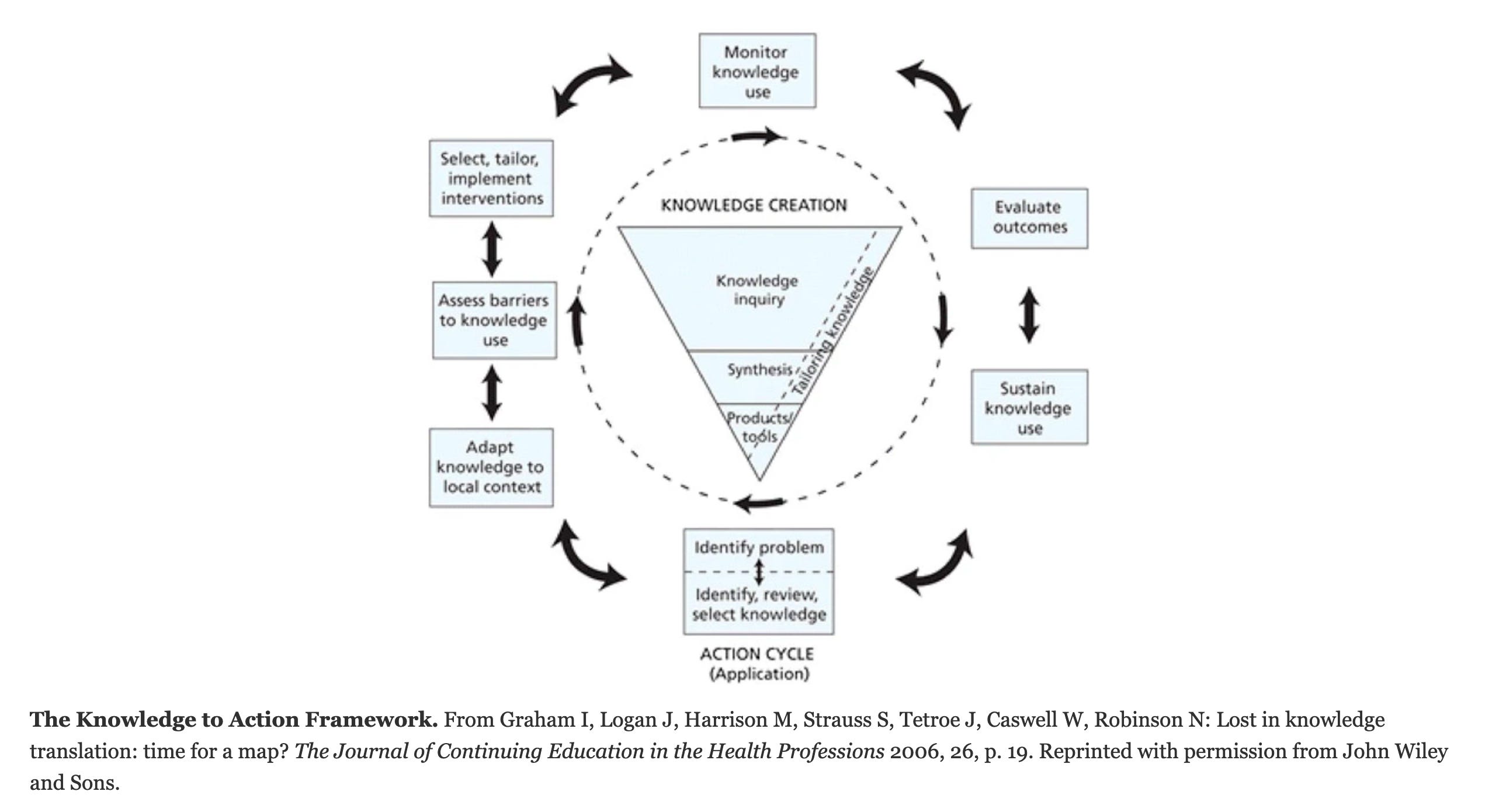
The framework describes the path from research to practice as consisting of two separate and distinct processes: knowledge creation and knowledge application.
Knowledge creation is largely the work of academia. Clinical trials and other studies are done, summarized, and eventually packaged in a format intended to facilitate their application in clinical practice.
The knowledge application cycle takes place in a local practice context. It starts when a problem is identified and a decision is made to fix it. Steps are then taken to identify a research-developed solution - a product or tool - that could improve the situation, adapt it for local use, and monitor how well it works.
A key insight provided by the KTA framework, that can be easily overlooked, is that there is no direct connection between knowledge creation and the knowledge application cycle, another words there is a missing link:
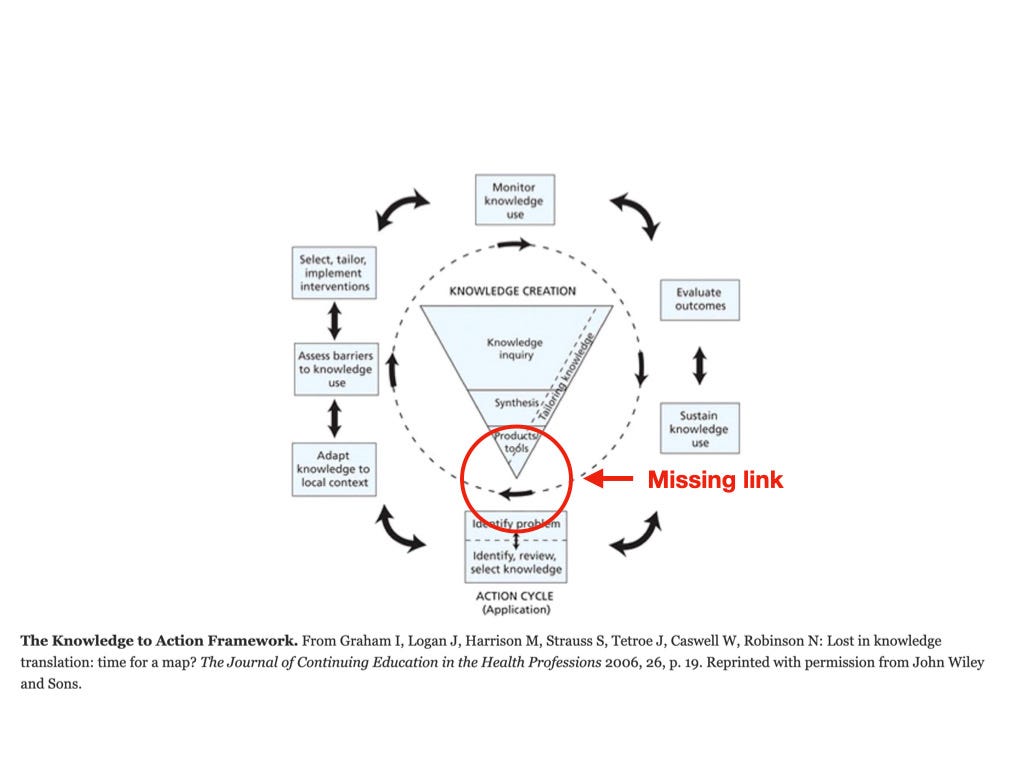
Thus, one has to ask the question, how do research-based findings and products cross this gap?
It is easy when the research-based findings and/or products meet an urgent clinical need. A good example is the new vaccines and treatments for COVID-19. But most often, clinical practices in need of improvement are less obvious. In this more common situation, I think there are several ways research products could cross the gap that could work independently, additively, or even synergistically.
The products could be actively “pushed” from within the knowledge creation sphere. For example, clinical practice guidelines created by specialty societies and others. These guidelines summarize research information and, if done well, clearly state a rationale and method for adapting current practice to reflect the current research findings.
The products could be actively “pulled” by clinicians seeking to improve the quality of their practice. This was the original idea behind evidence-based practice.
In addition to these two mechanisms that operate within the health care context, there could be external forces seeking to push the information from research into practice. An example is the mandate by the US Center for Medicare Services (CMS) requiring elements of shared decision making before approving payment for lung cancer screening. [4] Another example is a health care insurer establishing quality of care targets that must be met to avoid some sort of practice penalty.
As discussed in recent blog posts, there have been many attempts trying to push SDM into clinical practice. Numerous articles have been published in academic journals, SDM is becoming increasingly included in clinical practice guidelines, and there are several mandates imposed by external agencies (such as CMS discussed above). The evidence to date suggests that none of these efforts has made much of a difference. In KTA terms, this situation suggests the way forward is not to continue to create more SDM tools/products but to identify and address issues that inhibit their use in practice starting with how to cross the gap between the academic world of knowledge creation and the applied world of clinical practice.
Perhaps the way forward depends on our ability to interest clinicians in learning how to incorporate SDM into clinical care and motivate them to do so. If so, the keys to improving SDM use would be: first helping local practices recognize they should incorporate SDM into routine patient care and then helping local practice leaders identify appropriate SDM products/tools and then adapting them for use in their setting.
Do we have methods for accomplishing these tasks? If not, are they being developed? Are these steps even possible or will they first require a more fundamental transformation of the current culture of clinical care? Food for thought.
References
1. Schrager S, Phillips G, Burnside E. Shared decision making in cancer screening. Family practice management. 2017 May;24(3):5.
2. IOM (Institute of Medicine). Washington, D.C: National Academy Press; 2001. Crossing the Quality Chasm: A New Health System for the 21st Century
3. Graham ID, Logan J, Harrison MB, et al. Lost in knowledge translation: Time for a map? J Contin Educ Health Prof. 2006;26(1):13-24. doi:10.1002/chp.47
4. Merchant FM, Dickert NW Jr, Howard DH. Mandatory Shared Decision Making by the Centers for Medicare & Medicaid Services for Cardiovascular Procedures and Other Tests. JAMA. 2018 Aug 21;320(7):641–2.
This article was also published on MDM Musings, a SubStack newsletter.

Comments
Post a Comment